
Quick Answer: HA girth filler lasts ~12–48 months (maintained with small top-ups). Bellafill® (PMMA) is permanent, PERM® fat transfer is life-lasting, and surgical lengthening is a permanent anatomic change (traction and scar-care in weeks 1–8 determine how much visible length you keep). If you like your HA result, FusionThick™ can convert it to a permanent collagen scaffold.
- HA fillers: typically 12–48 months depending on product, metabolism, and aftercare; maintenance top-ups extend results.
- Bellafill® (PMMA): life-long collagen scaffold surrounding microspheres; touch-ups only for symmetry or additional size.
- MAXL® (non-surgical lengthening protocol): length gains are durable if post-program traction is followed; small regression if you stop.
- Surgical lengthening (MegaMAXL® / repositioning): structural change—permanent; final visible length depends on adherence to traction and scar management.
- Fat transfer (PERM® / PERMMAXL®): engineered for life-lasting thickness after integration; early variability during take-rate phase.
Table of Contents

Penis Enlargement Longevity: What’s Temporary vs. Permanent
If you’re comparing penis enlargement options, one question rises to the top: how long do results actually last?
The honest answer is that longevity depends on what changes the tissue (temporary gel vs. collagen scaffold vs. structural surgery), how precisely it’s performed, and how closely you follow aftercare in the first few weeks.
In this guide, we sort options into three durability buckets—temporary, durable, and permanent/life-lasting—and explain why each behaves the way it does over time.
Temporary hyaluronic acid (HA) fillers gradually metabolize but can be maintained with small, planned top-ups. Permanent stimulators like Bellafill® (PMMA) build a stable collagen scaffold that doesn’t “wear off,” though you can refine symmetry or add volume later.
Lengthening approaches range from program-based remodeling (MAXL) to anatomic change (surgical lengthening with repositioning); both can deliver long-term gains when traction and scar-care are done correctly.
Fat transfer using our PERM method is engineered for life-lasting girth once the graft has integrated.
Across all categories, outcomes improve when you pair urology-led technique with smart aftercare: traction as directed, post-surgical edema control, activity restrictions, and (for girth work at our clinic) circumcision prior to treatment to reduce migration and disease risk and enhance long-term aesthetics.
Use the TL;DR above and the Longevity Matrix below for quick answers, then dive into the sections below to see the typical timelines, what can shorten—or extend—results, and when a light “refresh” makes sense.
How long different enlargement options last
| Procedure | Typical Longevity | What Affects It | Maintenance |
|---|---|---|---|
| HA Girth Filler | 12–48 months | Technique, metabolism, activity, aftercare | Touch-ups 6–24+ mo |
| Bellafill (PMMA) Girth Filler | Permanent | Collagen response, technique | Optional refinements |
| MAXL Program | Durable | Patient compliance, tissue response | Optional light ongoing traction |
| Surgical Lengthening (MegaMAXL / repositioning) | Permanent | Postop traction, scar control, body habitus | None beyond early phase |
| PERM (Fat Transfer) | Life-lasting | Take rate, edema resolution, weight change | Occasional contouring if desired |
| PERMMAXL (Length + PERM) | Permanent length + life-lasting girth | Adherence to aftercare protocols | Rare refinements |
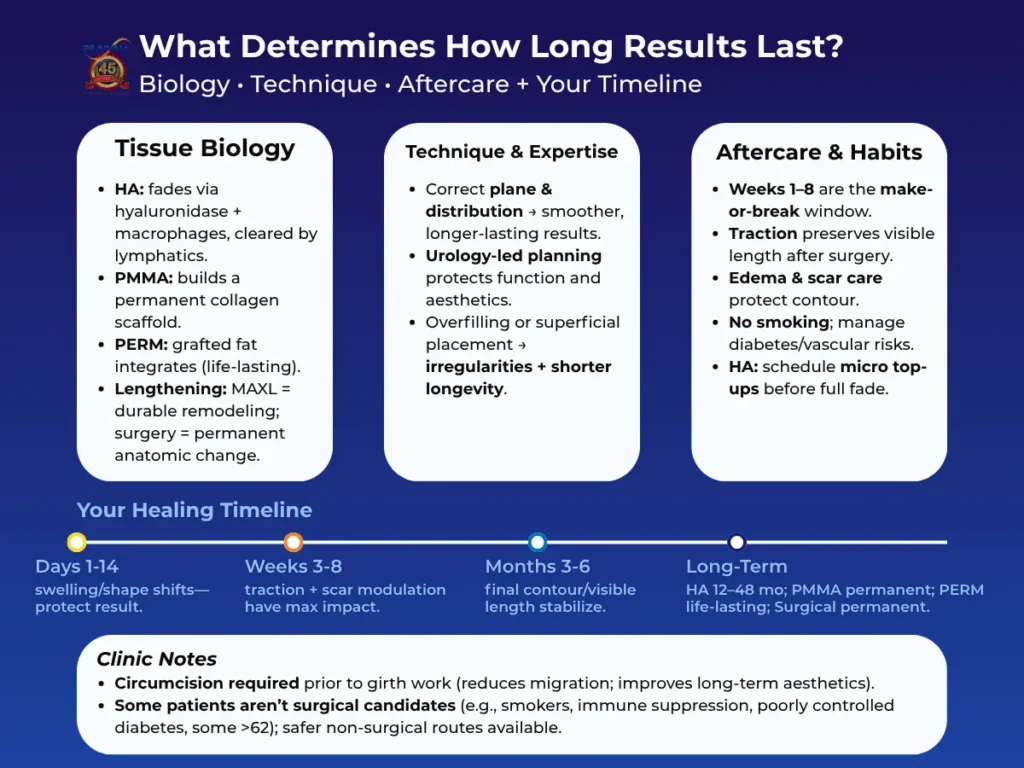
What determines how long results last?
Longevity isn’t random. It comes down to three things working together: what type of change you make in the tissue, how precisely it’s done, and how your body heals in the first few weeks.
Think of it like building a deck: the material you choose, how skilled the builder is, and how you protect it right after installation all influence how long it stays straight and strong.
1) Tissue biology: what your body does with the change
Hyaluronic acid (HA) fillers – temporary, maintainable
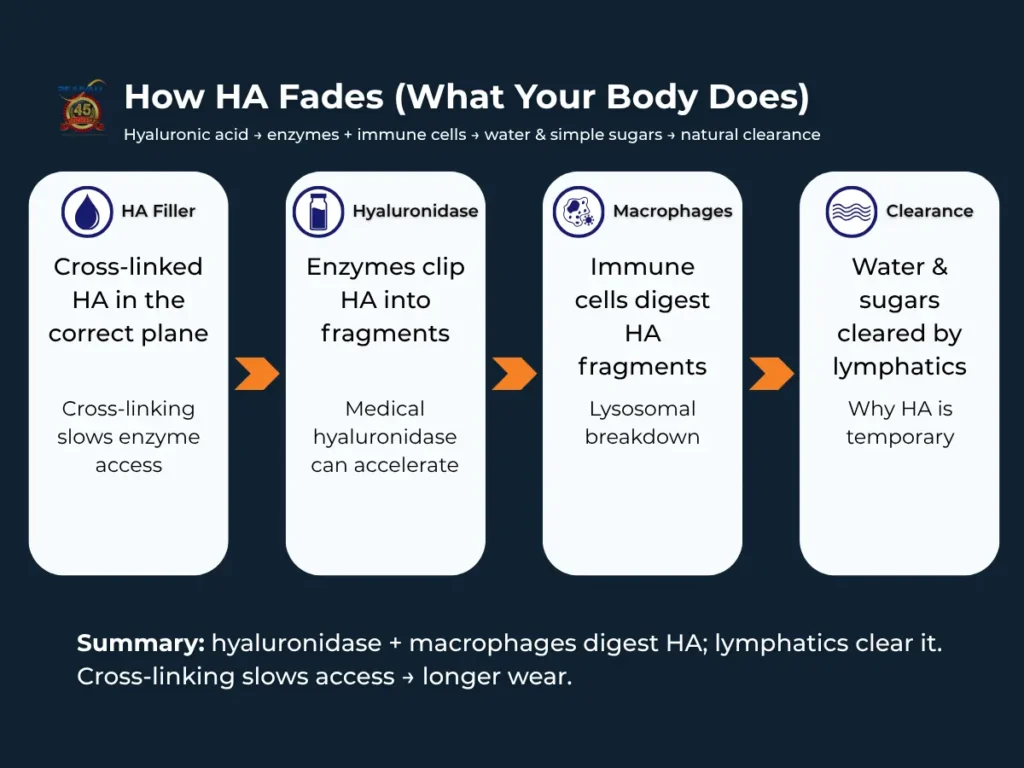
HA is a smooth gel your body can gradually break down with macrophages. Cross-linking (how tightly the gel is bonded) and where it’s placed influence how long it stays and how natural it feels.
With a good product and technique, most men enjoy 12–48 months of visible girth before noticing tapering.
HA is a sugar gel your body recognizes. Over time, natural hyaluronidase enzymes and immune cells called macrophages gradually digest it into water and simple sugars, which your lymphatic system clears. Cross-linking slows enzyme access, so better-engineered HA lasts longer.
Because HA fades slowly, small, planned top-ups keep you in your target size without dramatic swings. Because HA fades slowly, small, planned top-ups keep you in your target size without dramatic swings. Alternatively, at Rejuvall you can add Bellafill® (PMMA) to make the gains you made with HA permanent.
Bellafill® (PMMA) – a scaffold your body keeps
PMMA doesn’t “fill” forever by itself; instead, the microspheres prompt your body to build new collagen around them, creating a stable framework.
After the early settling phase, this scaffold is permanent. You don’t “lose” PMMA like HA—touchups are optional and usually for symmetry or to add more volume by choice.
Fat transfer (PERM) – living tissue that stays
In our PERM method, we transplant your own fat in a proprietary way that encourages high “take rate.” Once the grafted tissue reconnects with your blood supply and integrates, it behaves like fat anywhere else on your body—life-lasting.
Early weeks can show significant swelling (edema) and minor irregularities while things settle; then the contour stabilizes.
Lengthening – remodeling vs. anatomic change
- MAXL (non-surgical program): Gentle, consistent traction and a structured protocol create durable tissue lengthening and girth expansion over time. If you keep up with light maintenance traction, gains are maintained; if you stop completely, expect very minor regression toward baseline.
- Surgical lengthening (MegaMAXL with repositioning): The internal attachment is released, and the penis is repositioned, which is an anatomical, permanent change. The amount of visible length you keep depends on how the scar forms and whether traction guides healing in those first weeks.
2) Technique & provider expertise: why “how” matters as much as “what”
Penile tissue isn’t the face or lips; it has unique anatomy and function with complexity similar to the heart. A urology-led approach plans the correct plane of placement, volume per pass, and distribution so the result looks and feels natural and lasts.
- Correct plane = smoother, longer-lived results. Too superficial can create ridges or visible product; too deep wastes volume where it won’t show and damages the organ.
- Volume and passes matter. Overfilling in one session can stress tissue, increase swelling, and paradoxically shorten longevity by provoking unnecessary inflammation.
- Surgical finesse protects length. During lengthening surgery, meticulous handling of ligaments, bleeding control, and precise repositioning reduce scar tethering that can pull gains back.
Bottom line: The same product or procedure can age very differently in two different hands. Expertise shows up years later.
3) Aftercare & the “make-or-break” window (first 4–12 weeks)
Healing has a rhythm. The more closely you follow the plan in this window, the more of your gains you “lock in.”
- Traction (lengthening). Traction isn’t optional, it tells the healing tissue where to settle. Done correctly and consistently, it preserves the length you see on the table.
- Edema and scar control. Elevation, compression (when prescribed), anti-inflammatory protocols, and gentle tissue work (massage, rolling) at the right time reduce scarring that can steal length or distort girth.
- Activity restrictions. High-pressure activities (early sex, intense workouts, heavy lifting) can shift product, worsen swelling, or affect graft take. Waiting a few extra days is much cheaper and less painful than a revision.
- Planned maintenance for HA. Rather than waiting for complete fade, we can schedule micro-top-ups to keep you in your target zone with minimal downtime.
Think of the first month like wet cement: shape holds best if no one steps in it.
4) Your baseline & habits: the “you” factors that affect longevity
- Circumcision status. Our clinic requires circumcision before girth enhancement. A foreskin can act like a sleeve that encourages migration or unevenness; removal improves stability and aesthetics long-term. Dr. Carney is able to perform a girth-optimizing circumcision prior to enhancement.
- Body composition & weight change. After PERM, major weight loss or gain can globally change visible girth to a small degree.
- Smoking. Smoking (cigarettes, vapes, cannabis) constricts blood vessels and slows healing—this increases complications and can compromise final contour or length.
- Medical factors. Diabetes control, vascular health, aging, sleep apnea, and certain meds (e.g., anticoagulants) affect swelling, infection risk, and scar behavior.
- Realistic goals & compliance. The men who keep the best results are the ones who follow the prescribed aftercare plan and choose procedures that match their lifestyle and healing profile.
5) What the timeline really looks like (so you know what’s normal)
- Days 1–14: Expect swelling and shape changes. Protect the area, follow meds, and do not test the result early.
- Weeks 3–8: Tissue stabilizes. For lengthening, traction and scar modulation do the most good here. Small asymmetries often soften on their own.
- 3–6 months: Final contour and visible length settle. This is when we judge whether a tiny HA top-up or contour polish (if desired) makes sense.
- Long term:
–HA: gradual taper over 12–48 months; micro-top-ups keep you steady.
–PMMA: permanent scaffold; refinements are elective.
–PERM: life-lasting girth after integration; major weight swings can shift volume.
–Lengthening: permanent anatomic change; good early traction = more visible length kept.
Quick myths vs. facts
- “Permanent means I never need anything again.” Permanent tissue changes (PMMA scaffold, surgical lengthening, PERM) don’t fade—but you might still choose a small refinement for symmetry or preference.
- “If I feel great at 2 weeks, I’m healed.” Feeling better ≠ tissue stability. The month-1 to month-3 window is where patience pays off.
- “More product = more longevity.” Not always. Overfilling in one go increases swelling, lumps, and can shorten longevity by provoking scarring or irregularities.
How long do non-surgical girth injections last?
Non-surgical girth enhancement covers two main approaches: Hyaluronic Acid (HA) gel and Bellafill® (PMMA), a permanent collagen stimulator.
Many men start with HA to “test-drive” size and feel, then transition to a permanent result with our FusionThick protocol (adding PMMA to existing HA under strict technique). Here’s how longevity plays out—and how to keep results looking natural over time.
HA fillers: temporary but maintainable (12–48 months)
What to expect. HA is a smooth, body-friendly gel. It delivers a natural feel and a reversible on-ramp for first-timers. Most men enjoy 12–48 months of visible thickness before gradual tapering. Where you land in that range depends on the product chemistry, placement plane, volume, metabolism, and aftercare.
How it fades: Your own hyaluronidases and macrophages slowly digest HA into water and sugars that are cleared by your lymphatics; if needed, we can accelerate this with medical hyaluronidase.
How to extend results.
- Plan micro top-ups every 6–24+ months before full fade; this keeps you in the target zone without big swings.
- Protect shape early: limit high-pressure activities (sex, intense exercise) until cleared; follow edema control instructions.
- Remember: at our clinic, circumcision is required before girth enhancement to reduce migration risk and improve long-term aesthetics.
Who it suits. Men who want a reversible trial, prefer minimal downtime, or need a size “proof of concept” before deciding on permanence.
Bellafill® (PMMA): permanent collagen scaffold (life-long)
What to expect. PMMA microspheres don’t dissolve; they stimulate your body to build stable collagen around them. After the early settling phase, girth is permanent. Touch-ups are optional—typically to fine-tune symmetry or add more volume by preference, not because it “wears off.”
Longevity essentials.
- Technique matters: correct plane, distribution, and urology-led anatomy respect are key for smooth, long-term results that preserve function.
- Aftercare: early swelling is normal; gentle tissue work with massage and rolling at the right time helps polish contour.
Who it suits. Men ready for a lasting outcome who value low maintenance over time.
FusionThick™: make an HA result permanent without starting over
Many men start with HA to “test-drive” size and feel, then transition to a permanent result with our FusionThick™ protocol (adding Bellafill® (PMMA) to existing HA under strict technique).
How it works.
- Dr. Carney evaluates your current HA placement and contour, then layers PMMA strategically so your body replaces the temporary volume with your own collagen over time.
- Because the PMMA is added where the HA already “proved” your preferred size and shape, you avoid guessing and preserve the aesthetic you like, now with permanence.
Candidacy & timing.
- Best when HA is stable, smooth, and fully settled (no active swelling or recent large top-ups).
- Requires the same medical screening and aftercare diligence as standalone PMMA.
- As with any girth work at Rejuvall, circumcision is required.
Why patients choose FusionThick.
- Keeps the current look you already like
- Eliminates routine HA top-ups
- Reduces “trial-and-error” because your target contour is known
- Greatly lowers risk of granuloma associated with PMMA
What shortens or extends non-surgical longevity?
Shortens longevity / increases risk
- Early high-pressure activity (sex, vigorous exercise) before clearance
- Poor plane/overfilling in one session → swelling, irregularities
- Smoking (any form): impairs blood flow and healing
- Uncontrolled diabetes/vascular disease → slower recovery
Extends longevity / polishes outcomes
- Follow edema and scar-modulation steps precisely in weeks 1–8
- Schedule small, pre-emptive HA top-ups rather than large, infrequent ones
- Choose a urology-led injector who understands penile anatomy and function
- For permanence, consider PMMA or FusionThick once you love your size
Real-world timelines
- HA: smooth, natural feel immediately; shape “settles” over 2–6 weeks; 12–48 months of visible thickness; plan micro top-ups to avoid yo-yo sizing.
- PMMA: early settling in the first few weeks; collagen scaffold consolidates by 3–6 months; permanent thereafter, with optional refinements.
- FusionThick: uses your stable HA result as the blueprint; after PMMA layering, expect a similar early settling window and then permanent maintenance of your preferred contour.
Quick chooser: which path fits your goals?
- “I want to try this and keep it reversible.” → Start with HA and plan micro top-ups.
- “I’m ready for a stable, low-maintenance result.” → Bellafill® (PMMA).
- “I love my current HA look and want it to stay, permanently.” → FusionThick™.
Not sure which is right for you? Start with a free consultation.
Are surgical lengthening results permanent?
Short answer: Yes. Surgical lengthening (e.g., MegaMAXL with penile repositioning) creates an anatomic change that doesn’t “wear off.” What varies patient-to-patient is the amount of visible length you keep, which depends on scar behavior, traction, body habitus, and how closely you follow aftercare in the first 8–12 weeks.
What the surgery actually changes
- Internal release + repositioning. The internal attachment is released, and the penis is repositioned so more of the shaft sits externally. That’s why the change is permanent—you’re not stretching a temporary tissue; you’re altering where the penis rests.
- Why traction still matters. There is no such thing as surgery without scarring, and that goes for surgery of any kind, be it urologic or otherwise. During healing, collagen wants to contract. Traction guides the scar so the penis heals in the lengthened position, preserving visible gain.
Typical Timeline
- Days 1–14: Swelling and protective dressings. Short, gentle traction sessions begin when instructed. No “testing” the result early.
- Weeks 3–8: Scar is active; this is the make-or-break window. Consistent traction and scar modulation protect length.
- Months 3–6: Scar softens; visible length stabilizes. Most men see their true baseline here.
- Long-term: The anatomic change is permanent. Occasional soft tissue work (if advised) can further polish comfort and hang.
What influences how much visible length you keep
- Traction consistency & technique. Correct device, correct tension, correct instruction, and daily consistency matter much more than “more force.”
- Scar biology. Some men scar “tighter” than others; guided scar care (arnica, massage timing, Rx when indicated) helps.
- Pubic fat pad & skin. A large fat pad or tight skin envelope can visually “hide” length; candidacy may include mons reduction or tummy tuck for best visibility.
- Baseline anatomy & curvature. Pre-existing curvature, micropenis diagnosis, or buried penis changes treatment planning and expectations.
Combining length + girth (and when to do it)
Many men pair lengthening with girth for balance—either staged or in one plan (PERMMAXL when adding PERM fat transfer). Staging can be advantageous if you want to lock in visible length first, then fine-tune circumference and contour.
Safety, candidacy, and realistic goals
- Surgical enhancement is not for everyone. We screen out or optimize higher-risk patients (e.g., active smoking, immune suppression, poorly controlled diabetes, some men >62, etc.) because healing quality determines results. If surgery isn’t ideal, we’ll discuss MAXL or non-surgical girth options with clearer safety margins.
- Results are permanent, but your participation (traction, activity limits, follow-ups) is essential. “Set-and-forget” is not realistic in weeks 1–8.
Why provider expertise changes long-term outcomes
Rejuvall is led by Kenneth J. Carney, MD, PHARM, FACS, a world renowned board-certified urologist, plastic surgeon, and pharmacist who has specialized in penile enhancement and reconstruction for decades.
A urology-based approach protects erectile function and sensation while optimizing aesthetics—key reasons our lengthening results remain stable after the scar matures.
Dr. Carney also regularly performs revision surgery for men treated elsewhere, which informs how we prevent tethering, lost length, and contour issues in the first place.
What “permanent” looks like in real life
- You should expect a lasting change in hang and visible shaft length.
- The exact number you see in the mirror depends on adherence to the protocol and individual scar behavior.
- Rejuvall offers specific length guarantees for qualified surgical candidates; ask during your consult how those apply to your anatomy and plan.
Who may not be a candidate for surgery (and why healing matters)
Most men do well with urology-led surgical enhancement, but some patients face higher risks of wound-healing problems, infection, scarring, or poor cosmetic outcomes. We carefully screen for:
- Active smoking (cigarettes, vaping, cannabis). Smoking constricts blood vessels and impairs healing; cessation is typically required pre- and post-op.
- Immune deficiency or immunosuppressive therapy. Reduced infection control and slower tissue repair.
- Age over ~62. Not an absolute cutoff, but older patients often have slower healing and higher complication risk; eligibility is case-by-case after medical clearance.
- Poorly controlled diabetes (e.g., elevated A1c) or vascular disease. Increased risk of infection and delayed healing.
- Anticoagulants that can’t be safely paused, bleeding disorders, or significant cardiovascular issues without clearance.
- Active skin or urogenital infections, untreated STIs, or dermatologic conditions at the surgical site.
- BMI extremes, significant nutritional deficits, or sleep apnea not managed—each can worsen peri-operative risk.
- History of problem scarring (e.g., keloids) or connective-tissue disorders—relative risks discussed at consult.
- Low likelihood of aftercare compliance (traction, scar care, activity restrictions). Surgical results depend on it.
- Unrealistic goals or body-image concerns that surgery cannot resolve.
Clinic note: If you’re in a higher-risk group, non-surgical pathways (e.g., MAXL or carefully selected girth options) may be safer alternatives. We’ll guide you to the option that protects both function and aesthetics.
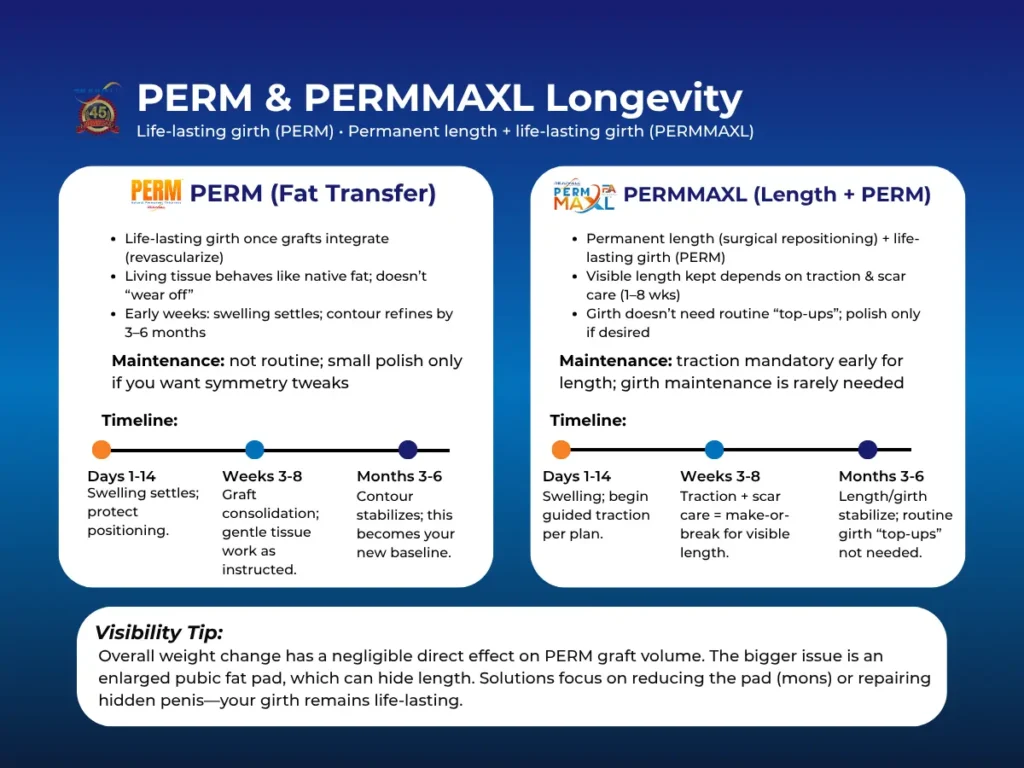
How long do PERM® and PERMMAXL® results last?
Short answer: After integration, PERM® girth gains are life-lasting because the grafted fat becomes living tissue. When combined with surgical lengthening (PERMMAXL), you get permanent length + life-lasting girth—with the final look shaped by early aftercare.
Why PERM is designed to last
- Living tissue, not a temporary filler. PERM transplants your own fat using a technique optimized for high take rate. Once the grafts revascularize (connect to your blood supply), they behave like native tissue and don’t “wear off.”
- Early weeks are a settling phase. Expect swelling (edema) and contour evolution as the grafts take. Irregularities usually soften as edema resolves and tissues knit.
Real-World Timeline
- Days 1–14: Swelling and firmness are expected. Protect the area; follow positioning and edema control instructions.
- Weeks 3–8: Grafts consolidate; contour refines. Gentle tissue work (when instructed) helps evenness.
- 3–6 months: Final circumference and feel stabilize. Most men consider this their new baseline.
- Long term: Life-lasting girth. Small polish procedures are elective and based on preference (e.g., subtle asymmetry), not because volume fades.
What actually affects the result
- Technique & plane selection. Urology-led placement in the correct planes supports smooth, natural contours that endure.
- Aftercare discipline. Edema control, activity restrictions, and timing of tissue work reduce complications and protect shape.
- Baseline skin & fat quality. Adequate skin and healthy fat tissue help the graft sit evenly.
About weight change (what patients get wrong)
- Overall weight gain/loss has a negligible direct effect on penile graft volume. Unlike large fat deposits elsewhere, the grafts in the penis don’t noticeably grow or shrink with typical weight swings.
- What does change the look is the pubic fat pad. Significant weight gain can enlarge the fat pad, visually burying the penis (hidden/buried penis). Your girth remains, but less shaft is visible. If this occurs, solutions may include fat pad reduction (mons) or, in complex cases, buried-penis repair—both of which restore visibility, not graft volume.
PERMMAXL: length + PERM in one plan
- What you get: Permanent length (from surgical release + repositioning) and life-lasting girth (from PERM).
- Why sequencing matters: Some men stage procedures—lock in visible length first (with traction and scar care), then add girth; others choose a combined plan when appropriate. We’ll recommend the path that best protects function, aesthetics, and healing.
Maintenance & Refinements
- Not routine. PERM doesn’t need “top-ups” like HA.
- When we do polish: Minor contour smoothing or small volume adjustments—usually for symmetry or personal preference.
- Traction: Not required for girth alone, but mandatory for the lengthening component (PERMMAXL) during weeks 1–8 to preserve visible length.
Safety & Candidacy
- As with any surgery, we screen for factors that impair healing (e.g., smoking, immune suppression, poorly controlled diabetes, some patients >62). If risks outweigh benefits, we’ll discuss safer non-surgical paths.
- Clinic policy: Circumcision is required before girth enhancement to reduce migration risk and improve long-term aesthetics.
Options That Often Age Poorly Over Time
Some approaches can look good briefly but don’t hold up well—or can create problems that later require removal and reconstructive work. If your goal is a natural look and feel that stays stable for years, it’s smart to avoid the following:
1) Unapproved or Non-Indicated Injectable Materials
Why to avoid: Higher rates of chronic inflammation, migration, infection, firm nodules (granulomas), and skin breakdown. These materials often can’t be reliably reversed and may spread unpredictably.
Long-term pattern: Increasing firmness, discomfort, contour distortion, and in severe cases tissue injury that can require staged surgical correction.
Better alternative: Temporary HA (reversible) or long-term options like Bellafill® or PERM® performed with urology-led technique and aftercare.
2) Implant-Based Augmentation Devices (cosmetic sheath-style implants)
Why to avoid: Risk of capsular contracture, erosion, sensory changes, visible edges, and infection. Removal is common—and can disrupt the skin envelope, making revision harder.
Longevity reality: Even when early results look smooth, complications often increase over time with motion, friction, and tissue remodeling.
Better alternative: For durable girth, consider PERM® or Bellafill®. For visible length, consider MAXL® or surgical lengthening with repositioning (MegaMAXL®) when appropriate.
3) Overfilling, “Megadosing,” or Cosmetic-Only Placement
Why to avoid: Large, poorly distributed volumes or overly superficial placement can create ridging, waviness, blood-flow compromise, and shorter-lived results due to unnecessary inflammation and scarring.
Red flags: “One-and-done” extreme size promises, non-urology injectors, rushed dosing, and no structured aftercare plan.
Better alternative: Staged, urology-led dosing in the correct planes with planned maintenance (HA) or properly layered Bellafill®/PERM®.
4) DIY Protocols and Low-Quality Extenders
Why to avoid: Unsupervised traction or off-spec devices can cause internal scarring (fibrosis), numbness, curvature, and uneven gains.
Better alternative: If you’re pursuing non-surgical length, use a clinic-approved device with a structured MAXL-style protocol and follow-up.
5) Non-Medical “Fillers,” Threads, or Unproven Devices
Why to avoid: Non-indicated materials and techniques can trigger foreign-body reactions, deformities, and long-term tissue damage—often with limited safe correction options.
Better alternative: Stick to medically supervised options with established safety profiles: HA or Bellafill® performed by a urology-led team, or PERM® when life-lasting living tissue is appropriate.
How Rejuvall Helps You Avoid Revision Landmines
- Urology-led planning prioritizes function, sensation, and blood flow so results age well.
- Procedure matching: Temporary HA (12–48 mo) for reversibility, Bellafill® (PMMA) for permanence, PERM for life-lasting living tissue, and lengthening (MAXL or surgical) when visibility—not just girth—is the goal.
- Revision expertise: We routinely treat complications from the options above; that experience informs how we prevent granuloma, migration, and contour loss up front.
Frequently Asked Questions
- HA girth filler: usually 12–48 months. Plan small, pre-emptive top-ups every 6–24+ months to avoid yo-yo sizing. It fades as hyaluronidases and macrophages break the gel into water and sugars that your body clears.
- Bellafill® PMMA girth filler: permanent collagen scaffold; refinements are optional (symmetry or added size).
- PERM fat transfer: life-lasting once grafts integrate; polish procedures are preference-based, not routine.
- MegaMAXL Surgical lengthening (ligament release + repositioning): permanent anatomic change; visible length kept depends on traction and scar behavior in weeks 1–8.
Yes—ask about FusionThick™. We strategically add Bellafill® (PMMA) to a stable, well-settled HA result so your body builds a permanent collagen scaffold that preserves the look you already like. Candidacy requires stable HA, standard medical screening, and (for girth work at our clinic) circumcision.
We screen out or optimize higher-risk patients because healing quality determines outcomes.
Higher-risk groups include active smokers, those with immune deficiency/immunosuppression, poorly controlled diabetes/vascular disease, some adults over ~62, patients on anticoagulants that cannot be safely paused, those with active infections or untreated skin conditions, and anyone unlikely to follow traction/scar-care.
Non-surgical paths (MAXL, HA, PMMA, PERM) may be safer alternatives.
At our clinic, yes. We require circumcision before girth work to reduce filler migration, prevent disease, and improve long-term aesthetics and hygiene. We offer a circumcision prior to girth enhancement that optimizes the shaft skin so you can get the biggest size increase possible.
Not because they “wear off.” Refinements are typically for symmetry, small contour polishes, or additional size by preference. Many men never need them.
PERM grafts: overall weight change has a negligible direct effect on penile graft volume.
Visibility: significant weight gain can enlarge the pubic fat pad, burying the penis so less shaft is visible. Solutions address the fat pad (e.g., mons reduction) or, when indicated, buried-penis repair.
Scar tissue naturally contracts. Traction in weeks 1–8 tells the healing tissue where to set, preserving visible length. Think of it as a “cast” for the internal healing process.
We use micro top-ups timed before full fade—usually every 6–24+ months—so size remains steady with minimal downtime. Many patients later convert their favorite HA contour to Bellafill® PMMA (FusionThick™) for permanence.
Penile tissue has unique anatomy and function with complexity similar to that of the heart. A urology-led approach plans plane, volume, distribution, and aftercare so results age well without compromising function.
Rejuvall is led by Kenneth J. Carney, MD, PHARM, FACS, a board certified urologist, plastic surgeon, and pharmacist who specializes in enhancement and reconstruction; we also manage complex revisions, which informs how we prevent problems upfront.
For qualified candidates, we offer specific length guarantees for surgical lengthening. Ask during your consultation how they apply to your anatomy and plan.
Follow your individualized plan; timelines vary by procedure. As a general guide:
- HA/Bellafill® (PMMA) girth: avoid high-pressure activity until cleared; early over-pressure can shift product or worsen edema.
- PERM®: allow grafts to consolidate; we’ll clear activities in stages.
- Surgical Lengthening (MegaMAXL®, SuperMAXL®): traction and scar-care dictate pacing; don’t “test” the result early—protect weeks 1–8.
Conclusion / Next Steps
Longevity isn’t luck—it’s biology, technique, and aftercare working together.
Temporary HA gives you a reversible on-ramp (12–48 months) with micro top-ups; Bellafill® (PMMA) and PERM® create stable, long-term girth (permanent/life-lasting); and surgical lengthening changes anatomy permanently when traction and scar-care are followed.
If you already love your HA look, FusionThick™ can convert it to a permanent collagen scaffold without starting over.
MAXL® non-surgical lengthening can increase length by about 1 inch and increase girth over half an inch without the need for scalpels and anesthesia.
What to do now:
- Skim the Longevity Matrix to match your goals and tolerance for maintenance.
- Book a consultation by filling out the form below to confirm candidacy (especially for surgery) and get a plan for aftercare and timing.
- If you’re not a surgical candidate today, we’ll map a non-surgical route that protects function and aesthetics—and keeps the door open for later options.
If the Cosmetic Urology Assessment form doesn’t appear above, click here to open it in a new window.

Dr. Steven L. Morganstern, M.D.
Dr. Morganstern is an internationally acclaimed, board-certified urologist, surgeon, and best-selling author specializing in men’s sexual health. A pioneer in erectile dysfunction therapeutics, Dr. Morganstern was the only private clinician selected for the original Viagra trials and has spent over four decades advancing treatments in ED, cosmetic urology, hormone replacement, and prostate health.